

















The study titled “Epidemiology of Dengue Fever in Somaliland: Clinical Features, and Serological Patterns from a Retrospective Study” aims to provide detailed information on dengue fever in Somaliland, a country where the disease is not well understood. Conducted by Dek Kahin Yosef and colleagues, it analyzes individual data from 1,410 suspected dengue cases at public hospitals between January and September 2024.
As of October 2023, Somaliland is facing a significant dengue fever outbreak, especially in the Hargeisa, Borama, and Gabiley districts. The Somaliland Ministry of Health has notified the WHO, confirming numerous positive cases through rapid diagnostic tests (RDTs).
Key points about dengue fever in Somaliland:
-
Recent surge: A marked increase in dengue cases has been noted since October 2023.
-
Affected areas: Hargeisa, Borama, and Gabiley are the most impacted regions.
-
WHO response: The WHO assists the Ministry of Health with field investigations, supplies RDT kits, and enhances the diagnostic capabilities of healthcare workers.
-
Testing and confirmation: Cases are confirmed using rapid diagnostic tests.
-
Community awareness: Initiatives are underway to educate communities about dengue prevention.
Globally, dengue fever is a critical public health concern, but its epidemiology in Somaliland is not well understood. This study aims to provide detailed data on the clinical presentation, demographic characteristics, and serological patterns of dengue in the country.
The study offers essential insights into Somaliland’s dengue epidemiology, revealing unique features that differ from other areas. It emphasizes the urban concentration of cases, the disproportionate impact on adults, and the prevalence of acute infections, highlighting the need for targeted interventions and improved surveillance.
These findings will inform future research and policy decisions, stressing the importance of enhancing vector control measures, diagnostic capabilities, and public awareness.
Despite certain limitations, this study serves as a foundation for more extensive investigations to fill knowledge gaps and develop effective strategies against dengue in Somaliland and similar contexts.
The insights gained contribute to a better understanding of dengue epidemiology in understudied regions and underscore the necessity of context-specific approaches in global dengue control initiatives.
Key Findings:
-
Out of the suspected cases, 175 (about 12.4%) tested positive for dengue.
-
The majority of positive cases were in males (60.6%) and individuals aged 19–38 years (45.1%).
-
Most confirmed cases came from urban areas (58.9%).
-
Common symptoms reported included fever, vomiting, nausea (86.7%), and gastrointestinal issues (86.1%).
-
Serological testing showed that 84.6% were positive for the dengue NS1 antigen, 8.6% for IgM antibodies, and 6.9% for both.
-
The peak incidence of cases occurred in June.
-
Only 8.7% of the patients required hospitalization, with half classified as severe cases.
Conclusion:
This study highlights the need for better understanding and surveillance of dengue in Somaliland, particularly in urban adults. The findings suggest a call for improved public health strategies and diagnostic practices, given the country’s limited data on the disease’s prevalence and transmission dynamics. Further research with larger sample sizes is necessary to validate these initial findings and improve dengue management in the country.
The full study is as follows:
Epidemiology of Dengue Fever in Somaliland: Clinical Features, and Serological Patterns from a Retrospective Study
By Dek Kahin Yosef, Ahmed Saeed Ismail, Barwaqo Saleban Awil, Halima Ahmed Hassan & Mohamed Ahmed Hassan
BMC Infectious Diseases
Volume 25, Article number: 179 (2025)
Published:
Abstract
Background
Dengue fever is a significant global public health concern. However, its epidemiology in Somaliland remains poorly characterized. This study aimed to provide comprehensive data on the clinical presentation, demographic characteristics, and serological patterns of dengue fever in Somaliland.
Methods
A retrospective analysis was conducted on 1,410 suspected dengue cases from public hospital laboratories in Somaliland between January and September 2024. Demographic data, clinical symptoms, and results of rapid diagnostic tests for dengue NS1 antigen and IgM antibodies were analyzed.
Results
Of the 1,410 suspected cases, 175 (12.41%) tested positive for dengue. The majority of the patients were male (60.57%) and aged 19–38 years (45.1%). Most cases were from urban areas (58.9%). Common symptoms included fever, vomiting, nausea (86.7%), GIT problems (86.12%) were the predominant symptom of patients. Serological testing revealed 84.57% NS1 positivity, 8.57% IgM positivity, and 6.85% positivity. The peak incidence was observed in June. Only 8.67% of the patients required hospitalization. Among these 8 cases (53.3%), as sever dengue and 7 (46.6%) were dengue with warning signs.

Conclusion
This study provides initial insights into the epidemiology of dengue in Somaliland, though further research is needed to establish robust baseline data, highlighting its prevalence, particularly in urban adults. These preliminary findings suggest a potential need for enhanced surveillance and public health measures, pending confirmation from larger studies to address the emerging arboviral diseases in this region.
Background
Dengue virus (DENV) presents a significant global health challenge, with an estimated 390 million infections occurring annually [1, 2]. This arbovirus, primarily transmitted by Aedes mosquitoes, causes dengue fever, a febrile illness that can progress to severe manifestations such as dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) [3, 4]. The global burden of dengue has been increasing, with Africa emerging as a region of growing importance despite limited data on seroprevalence [5]. Factors such as urbanization, climate change, and population mobility have contributed to the spread of dengue, necessitating a better understanding of its prevalence and associated risk factors in understudied areas [6, 7].
In Somaliland, the epidemiology of dengue fever remains poorly characterized, with significant gaps in the knowledge regarding its age-specific incidence, sex distribution, and seasonal variation. Previous studies conducted in 1989 and 2014 provided preliminary insights into the presence of dengue virus in the region, with seroprevalence rates ranging from 39 to 62% [8, 9]. However, these studies were limited by their small sample sizes, geographical scope, and lack of comprehensive clinical and serological data, leaving significant gaps in our understanding of the epidemiology of this disease.
The absence of detailed serotype prevalence data hinders the development of targeted vaccines and therapeutic interventions tailored to circulating dengue strains in Somaliland. Furthermore, reliance on rapid diagnostic tests (RDTs) with limited sensitivity not only compromises the accuracy of dengue diagnosis but also delays the initiation of appropriate clinical interventions, underscoring the critical need for investment in diagnostic infrastructure to improve patient outcomes.
The limited data on dengue seroprevalence and vector distribution in Somaliland not only impedes the formulation of effective vector control strategies but also complicates efforts to model disease transmission dynamics, which are critical for outbreak prediction and response planning. For instance, the lack of detailed epidemiological data during the 1989 dengue outbreak in Hargeisa, including age-specific seroprevalence and vector distribution, has impeded timely implementation of targeted vector control measures and public health interventions.
To address these critical knowledge gaps, this study aimed to provide comprehensive data on the clinical presentation, demographic characteristics, and serological patterns of dengue fever in Somaliland. By focusing on clearly defining the research gap, our study contributes new knowledge to the field by determining the age-specific incidence rates and sex distribution of dengue fever, investigating the seasonal variation in dengue cases, and evaluating the performance of current diagnostic methods, including RDTs, in the context of the limited resources in Somaliland.
The findings of this study provide crucial epidemiological data to inform targeted public health interventions, optimize diagnostic strategies, and guide future research efforts in Somaliland and similar resource-limited settings. By addressing these knowledge gaps, we aimed to contribute to the improvement of dengue prevention, diagnosis, and management in the region, ultimately reducing the burden of this important arboviral disease.
Methods
Study area and design
This study was conducted in Somaliland, an autonomous region of the Horn of Africa that claims independence. This area covers approximately 176,120 square kilometers (68,000 square miles) and shares borders with Bordered by Djibouti in the northwest, Ethiopia in the south and southwest, and Somalia in the east. The northern edge is defined as the coastline along the Gulf of Aden. The capital city is Hargeisa, Berbera serves as the main port, and Burao is an important urban area. This study employed a descriptive and retrospective approach, analyzing secondary data collected from public hospital laboratories between January 10 and September 5, 2024.
Study eligibility, population, and sample size
This study included all properly documented suspected dengue cases tested in public laboratories during the study period. Patients with incomplete serological profiles, clinical information, or sociodemographic data were excluded. This study included 1410 suspected dengue cases identified through systematic random sampling of public laboratory records over a specified period.
Diagnostic tool
All patients were tested for dengue rapid diagnostics for both NS1 and IgM markers using the SD Biosensor Dengue Duo NS1 Antigen and IgM Test Kit (Germany) at Somaliland Public Laboratories. The SD Biosensor Dengue Duo NS1 has a sensitivity and specificity of 92.98% and 98.7%, respectively, whereas Dengue IgM has a sensitivity and specificity of 72.0% and 83.5%, respectively.
Data collection instrument and process
The laboratory provided an Excel spreadsheet that contained this information. Data were extracted from the laboratory records by a trained team using a standardized data collection form designed for this study. The extracted data were then double-entered into an Excel spreadsheet to minimize entry errors. The collected data included demographic details (sex, marital status, age, place of residence, and geographical region), clinical manifestations, dates of testing, and outcomes of dengue IgM and NS1 rapid diagnostic tests (RDTs).
Data analysis
The collected data, which were initially stored in a Microsoft Excel spreadsheet, were thoroughly examined to identify and eliminate duplicate entries. The dataset was verified to be comprehensive, encompassing all relevant demographic information, testing dates, and serological outcomes. Following this initial process, data were transferred to Stata version 15 for further analysis. Descriptive statistics were then generated and frequencies and percentages were calculated and presented in tabular and graphical formats to provide a clear overview of the findings. Chi-square analysis was used to examine the association between clinical symptoms and hospitalization in patients with dengue. Statistical significance was set at P < 0.05.
Cramer’s V was used to measure the association between categorical variables, specifically clinical symptoms, and hospitalization status. This chi-square-based measure ranged from 0 to 1, with higher values indicating stronger associations. The Cramer’s V method is suitable for nominal data with multiple categories. Values were interpreted as: <0.1 negligible, 0.1–0.3 small, 0.3–0.5 moderate, > 0.5, large effect. This analysis quantified the relationship between symptoms and the likelihood of hospitalization.
Results
Sociodemographic variables
Out of the 1410 suspected individuals tested for dengue infection, 175 were found to be positive. The numbers of dengue-positive females and males were (n = 69, 39.43%) and (n = 106, 60.57%), respectively. Most dengue cases were 19–38 years (n = 79, 45.1%), followed by ≤ 18 years (n = 25, 14.3%), and ≥ 39 years (n = 71, 40.6%). The distribution of dengue-positive cases across regions included Togdheer (n = 52, 29.71%), Awdal (n = 50, 28.57%), Marodijeex (n = 45, 25.71%), and Sahel (n = 28, 16%). Regarding residence, most of the reported cases were from urban areas (n = 103, 58.9%), followed by rural areas (n = 72, 41.1%) (Table 1).
| Variables | Frequency | Percent |
|---|---|---|
| Sex | ||
| Male
female |
106
69 |
60.57
39.43 |
| Age | ||
| ≤ 18 years
19–38 years ≥ 39 years |
25
79 71 |
14.3
45.1 40.6 |
| Residence | ||
| Urban
Rural |
103
72 |
58.9
41.1 |
| Marital status | ||
| singles
married divorced |
24
148 3 |
13.71
84.57 1.71 |
| Regions | ||
| Togdheer region
Marodijeex region Awdal region Sahel region |
52
45 50 28 |
29.71
25.71 28.57 16 |
Clinical cases of dengue in Somaliland
In the clinical observation of dengue cases of infected patients in Somaliland, after excluding two cases of missing clinical symptoms, fever, vomiting, and nausea (n = 150, 86.7%), GIT problems (n = 149, 86.12%) were the predominant symptoms, followed by gastrointestinal symptoms, including abdominal pain (n = 107, 61.84%). Respiratory symptoms such as cough and chest pain were reported by (n = 137, 79.19%) of patients, while myalgia affected (n = 122, 70.52%), and headache (n = 134,77.45%) of cases, followed by Rash (n = 90, 52.02%) of the patients was observed. Notably, (n = 64, 36.9%) patients experienced neurological symptoms, including confusion, changes in consciousness, and occasional seizures (Table 2).
Serological profile of dengue in Somaliland
In 2024, 1,410 dengue suspected patients were examined, 175 cases were confirmed dengue positive. Among these (n = 15, 8.57%) individuals tested positive for dengue IgM, (n = 148, 84.57%) tested positive for dengue NSI, and (n = 12, 6.85%) tested positive for both NSI and IgM (Table 3).
| Variables | Frequency | Percent |
| Fever | 150 | 86.70 |
| Headache | 134 | 77.45 |
| Cough | 137 | 79.19 |
| Chest pain | 137 | 79.19 |
| Neurological symptoms (confusion, altered consciousness, and seizures) | 64 | 36.9 |
| Rash | 90 | 52.02 |
| Abdominal pain | 107 | 61.84 |
| GIT problem | 149 | 86.12 |
| Myalgia | 122 | 70.52 |
| Vomiting and nausea | 150 | 86.70 |

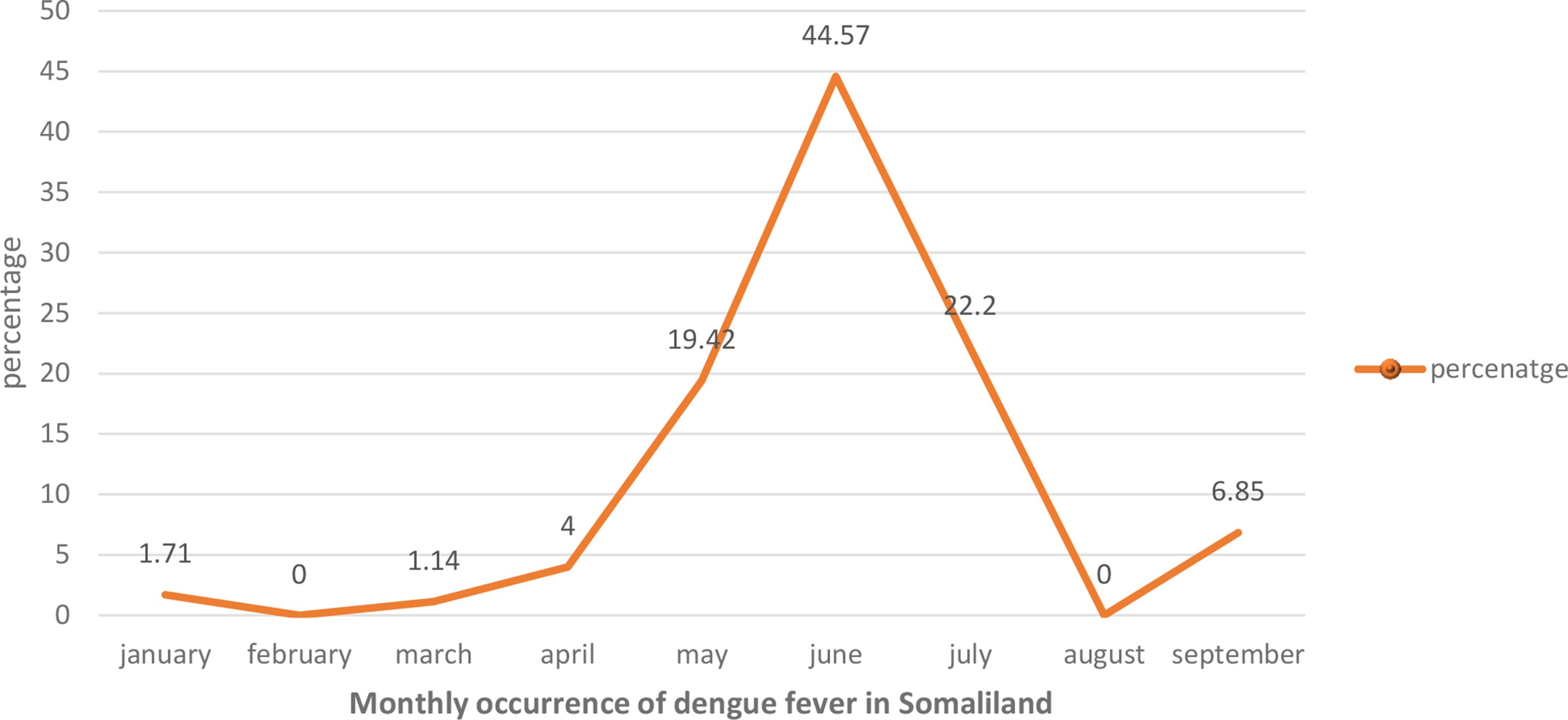
Illustrates the monthly occurrence of dengue fever in Somaliland. Visual representation illustrates the number of documented dengue fever cases
Severity of dengue fever in Somaliland
Only (n = 15, 8.67%) of patients required hospitalization, with a slight predominance of male patients among the severe cases. The age distribution of hospitalized patients suggested a potential correlation between increasing age and disease severity, with the majority of admitted patients aged ≥ 39 years (n = 8, 53.3%) (Table 4).
| Serological result | frequency | Percentage |
|---|---|---|
| Total dengue cases | 1410 | |
| Dengue positive cases | 175 | 12.41% |
| Dengue IgM positive | 15 | 8.57% |
| Dengue NSI positive | 148 | 84.57% |
| Both NSI and IgM positive cases | 12 | 6.85 |
Association between clinical symptoms and hospitalization of dengue patients in Somaliland
Chi-square analysis revealed that rash and myalgia were significantly associated with hospitalization (p = 0.013 for both) and had strong effect sizes (Cramer’s V = 0.644), indicating that these symptoms may serve as key indicators for hospitalization. Conversely, fever, headache, cough, chest pain, neurological symptoms, abdominal pain, and gastrointestinal problems were not significantly associated, although cough had a moderate effect size (Cramer’s V = 0.41); this merits further investigation (Table 5).
| Variables | frequency | Percent |
|---|---|---|
| Number of outpatients | 158 | |
| Warded | 15 | 8.57% |
| Sex | ||
| Male
Female |
10
5 |
66.6
33.3 |
| Age | ||
| ≤ 18 years
19–38 years ≥ 39 years |
2
5 8 |
13.3
33.3 53.3 |
| Symptom | Chi-Square Value (χ²) | Degrees of Freedom (df) | p-Value | Effect Size (Cramer’s V) |
|---|---|---|---|---|
| Fever | 1.22 | 1 | 0.268 | 0.28 |
| Headache | 0.26 | 1 | 0.605 | -0.13 |
| Cough | 12.63 | 1 | 0.104 | 0.41 |
| Chest pain | 0.010 | 1 | 0.91 | 0.026 |
| Neurological symptoms | 0.076 | 1 | 0.78 | 0.071 |
| Rash | 6.23 | 1 | 0.013* | 0.644 |
| Abdominal pain | 0.57 | 1 | 0.44 | 0.196 |
| GIT problem | 1.22 | 1 | 0.268 | 0.285 |
| Myalgia | 6.23 | 1 | 0.013* | 0.644 |
Discussion
This study provides initial insights into the epidemiology of dengue in Somaliland, though further research is needed to establish robust baseline data, highlighting its prevalence and distinct characteristics. This study involved 1,410 subjects with diverse sociodemographic backgrounds. The results revealed a 12.41% prevalence of dengue among positive cases, indicating its significant presence as a public health concern in Somaliland.
The number of males infected was 60.57%, which is higher than the female infection rate in our study, in contrast to the findings of previous studies, which reported a predominance of female subjects [10,11,12,13]. This gender disparity may be attributed to factors such as differences in exposure to mosquito vectors due to occupational or behavioral patterns or variations in healthcare-seeking behavior between males and females in the study population. In addition, we found that most infected dengue patients (45.1%) were 19–38 years of age, followed by those aged ≥ 39 years (40.6%). This finding is comparable to those of a study conducted in Thailand (40.69%) [14] and Singapore (50.8%) [15]. The high vulnerability of this age group to dengue in adult populations may result in elevated infection risks due to increased exposure to mosquito vectors during outdoor activities. Additionally, the clinical presentation and manifestations of the disease in adults are often more subtle and challenging to diagnose than those in pediatric cases [16, 17].
This study examined the prevalence of this disease across four distinct areas of Somaliland (Somalia). The findings revealed that most confirmed dengue cases were concentrated in the Togdher and Awdal regions, with the Marodijeex and Sahel regions also reporting infections (Table 1). The geographical distribution of the cases provides valuable insights into the spread of the disease within the country. The northwestern part of Somaliland, encompassing Awdal and Waqooyi Galbeed (Maroodi Jeex), has experienced a decline in precipitation and an increase in average temperature over the last 30 years.
These climatic shifts towards hotter and more arid conditions may influence the prevalence of mosquito-transmitted illnesses such as dengue fever, given that mosquito populations are responsive to environmental changes [18, 19]. The elevated incidence of dengue in Togdheer (Burao), Awdal (Borama), and Maroodijeex (Hargeisa) in Somaliland can be attributed to a multifaceted interaction involving mosquito ecology, human movement trends, and the capabilities of the local healthcare infrastructure.
The study found that of 175 confirmed dengue cases, 103 (58.9%) of dengue cases were from urban environments, compared to 72 (41.1%) from rural areas. This demonstrates the clear urban predominance of dengue cases in Somaliland. This supports findings from other regions [20,21,22]. However, contradictions have also emerged [23, 24]. Several factors may contribute to higher urban prevalence, including greater population density in cities, poor urban sanitation infrastructure, abundance of artificial water containers that serve as vector breeding sites, and increased human movement and interaction in urban areas. The contradictions in some studies could be due to regional variations in urbanization patterns, climate, vector ecology, or socioeconomic factors that influence dengue transmission dynamics.
Urban areas in Somaliland are struggling with water storage and waste management, thereby fostering the breeding of Aedes mosquitoes. Warmer city microclimates may lengthen the mosquito breeding season. Although specific studies of Somaliland are limited, research in other areas offers insights. For example, a study in Delhi found that lack of tap water access significantly increased dengue virus seropositivity [25]. In Brazil, inadequate sanitation is associated with a high incidence of dengue [26]. A Colombian study showed that monthly insecticide treatments in street catch basins significantly reduced the number of Aedes larvae and dengue cases (Ocampo et al., 2014). Effective environmental management, including proper sanitation, waste management, and water systems, has controlled disease vectors such as dengue [27]. In Guangzhou, China, artificial lakes have been linked to increased dengue outbreaks by providing additional mosquito breeding sites [27].
Patients with dengue often exhibit a range of clinical symptoms [28]. In our study, the most prevalent manifestations were elevated body temperature (86.70%) and gastrointestinal disturbances, such as emesis and nausea (86.70%) (Table 2). These findings align with those of previous studies of dengue symptomatology [29,30,31]. Other commonly observed symptoms in dengue cases include gastrointestinal issues (n = 150, 86.70%), myalgia (n = 122, 70.52%), and respiratory symptoms, such as cough and headache. This was Followed by chest pain (79.19%) and rashes (52.02%) [31,32,33].
The high prevalence of neurological symptoms (36.9%) observed in our study is a significant finding. In some cases, the neurological symptoms observed primarily included confusion, altered consciousness, and seizures. Our finding was higher than that of Carod-Artal et al. (2013), who found neurological complications in 21% of patients with dengue [34]. However, other studies have reported conflicting results. For instance, Kulkarni et al. (2021) reports a lower percentage, stating that “Of these, 154 (2.64%) had neurological manifestations,” [35] and a study conducted in India reports neurological complications due to dengue fever at 9.5%, with the most prevalent symptoms, each occurring in 73.3% (n = 22) of cases, being cephalalgia, impaired consciousness, and convulsions [35, 36]. This discrepancy could be attributed to differences in study populations, clinical settings, direct viral effects or diagnostic criteria used, and delayed healthcare-seeking behavior due to limited access to healthcare facilities, which can lead to the progression and exacerbation of neurological conditions.
In our investigation, the majority of dengue-positive cases were classified as mild and were managed on an outpatient basis. Fifteen patients (8.57%) required hospitalization. According to the World Health Organization classification [37], the primary cause of hospitalization was severe dengue, accounting for eight cases (53.3% of hospitalized patients), and dengue with warning signs, comprising seven cases (46.6% of hospitalized patients). Among these, two cases involved young individuals, whereas five cases were within the 19–38 age range. However, nearly half of the severe cases occur in adults aged ≥ 39 years, similar to those reported in Saudi Arabia [1] and India [2].
Our study found that a higher proportion of hospitalized patients were older (≥ 39 years). Although this observation suggests a potential correlation between increasing age and disease severity, it is important to note that our study did not explicitly examine the role of comorbidities in this relationship. Comorbidities such as diabetes, hypertension, and cardiovascular disease are more prevalent in older populations and are known to complicate dengue management and lead to poorer outcomes. Several studies have highlighted the association between comorbidities and increased severity of dengue infection such as diabetes, and patients with pre-existing diabetes were associated with dengue severity [38, 39]. The higher hospitalization rate among older patients in our study could be attributed age-related physiological changes affecting the immune response to dengue infection, a higher likelihood of comorbidities exacerbating the disease course, and potentially delayed healthcare-seeking behavior leading to more advanced disease at presentation. Dengue infection in children often results in severe vascular permeability and a sudden onset of shock [40, 41].
Our study revealed an unexpected finding regarding the severity of dengue cases among children in Somaliland. Contrary to established literature, which typically identifies children as a high-risk group for severe dengue [42, 43], we observed relatively few pediatric cases with severe symptoms. This discrepancy warrants careful consideration and may have important implications for understanding the dengue epidemiology in this region.
Several factors could explain this observation. First, our reliance on data from public hospital laboratories may have introduced a sampling bias, potentially underrepresenting pediatric cases treated in other healthcare settings or those not seeking formal medical care. Second, differences in care-seeking behavior among parents in Somaliland could result in fewer children with milder symptoms being brought to hospitals, thus skewing our sample towards more severe adult cases. Finally, it is possible that this finding reflects a genuine epidemiological trend unique to Somaliland, where adults may be more severely affected by factors such as circulating serotypes or population immunity profiles.
The study found an overall prevalence of 175 (12.41%), which was comparable to findings in Puntland state, Somalia (12.3%) [44], but lower than those reported in Sudan (42%) and Kenya (61.2%) [45, 46]. These variations could be attributed to differences in environmental factors, the size of the samples analyzed, and the methods used for diagnosis. The findings revealed that 8.57% of dengue cases tested positive for dengue IgM antibodies, which aligns with the 8% prevalence reported in Indian studies [47]. However, 28.32% reported from Mangaluru [48] and 14.7% in Italy [49], and this study revealed a significant occurrence (84.57%) of dengue NS1 antigen among the tested subjects which is almost close with study done from Puntland [44]. Detection of the NS1 antigen is particularly useful during the early stages of dengue infection, especially from the third to fifth day after symptom onset, when virus levels in the bloodstream may be too low for detection and the immune system has not yet produced sufficient anti-IgM antibodies for reliable identification [50]. These discrepancies are likely attributable to various factors including the timing of sample collection, differences in testing methodologies, diverse patient demographics, and specific dengue serotypes involved. The small percentage of cases (6.85%) showing both NSI and IgM positivity is likely due to the short time frame during which both markers can be simultaneously detected [51, 52].
This study identified significant correlations between clinical manifestations and hospitalization in patients with dengue, specifically focusing on rash and myalgia, corroborating previous research on the relevance of these symptoms in disease progression and severity [53,54,55]. The strong association between rash and hospitalization aligns with the findings of Tiga-Loza et al. (2020), who observed that rash persisting for a month after fever onset was prevalent among hospitalized patients [56]. This correlation was further substantiated by Santos et al. (2004) and Jelinek (1997), who recognized rashes as an indicator of severe dengue. The underlying pathophysiological mechanisms likely involve increased vascular permeability and immune-mediated processes.
The significant correlation between myalgia and hospitalization aligns with the findings of Suppiah et al. (2018) and Mallhi et al. (2015), who reported a higher prevalence of myalgia in hospitalized patients with dengue [57,58,59]. Interestingly, fever, a primary dengue symptom, showed no significant association with hospitalization, which is consistent with the results of other studies [60, 61]. This may be due to the timing of fever onset and emergence of severe symptoms.
Despite the moderate effect size for cough, which lacked statistical significance, further investigation is required. Respiratory symptoms are generally not linked to dengue; however, Rodrigues et al. (2014) suggested that pleural effusion may be more common in severe dengue cases than previously thought [62]. Increased pulmonary involvement could be due to the virus affecting multiple organ systems, the host inflammatory response, or complications from severe vascular leakage [63].
The lack of significant associations for symptoms, such as headache, chest pain, and gastrointestinal disturbances, is notable. These results contrast with those of Paraná et al. (2024), who found strong correlations between headache, chest pain, abdominal pain, and dengue severity [42]. This difference may stem from variations in sample size, study design, regional differences in dengue presentation, timing of symptom assessment, predominant virus serotypes or strains, healthcare accessibility, treatment protocols, and prevalence of comorbidities or confounding factors among the study populations.
In 2024, the dengue incidence reached its highest point in June, subsequently declined from August, and slightly increased in September (Fig. 1), potentially influenced by shifts in climate and precipitation patterns. Somaliland experiences temperatures ranging from 27 °C to 37 °C, with major rainfall periods occurring in spring (April–June) and fall (October–December) [64]. The fluctuations in dengue incidence observed on a monthly basis may be attributed to alterations in the climatic conditions and precipitation patterns. Climate variability has been shown to have a significant impact on the occurrence of dengue fever across multiple studies [65, 66].
This study provides insights into dengue fever occurrence in Somaliland; however, it has several limitations. The reliance on rapid diagnostic tests, which have limited sensitivity and specificity compared to more advanced methods such as PCR, may have affected the accuracy of case detection. The absence of data on circulating dengue serotypes limits our understanding of disease dynamics.
The study’s retrospective nature and focus on a single public hospital may not capture all cases, especially milder cases that do not seek hospital care. The short study period may not reflect long-term trends.
Additionally, the study did not incorporate climatic data, such as precipitation or temperature, which could have provided insights into seasonal patterns. The use of secondary data sources introduces potential issues of incompleteness or omission. Some cases lacked comprehensive clinical details and there was an absence of virological or genomic data. Long-term patient outcomes were not available, limiting the assessment of prognosis and treatment efficacy.
This study could not determine the origin of dengue infections or provide detailed information on disease transmission patterns. Despite these limitations, this study offers valuable preliminary data on dengue fever in Somaliland and establishes a foundation for future studies. To address these constraints, future research should prioritize primary data collection, including comprehensive clinical documentation, advanced diagnostic techniques for viral characterization, and collection of local meteorological data alongside dengue case data. Implementing a robust surveillance system to track case outcomes and transmission patterns would significantly enhance our understanding of dengue fever dynamics in this region.
Conclusion
This study provides crucial initial insights into the epidemiology of dengue in Somaliland, revealing distinct characteristics that differ from those of other regions. These findings highlight the urban predominance of cases, the disproportionate impact on adult populations, and the prevalence of acute infections, underscoring the need for targeted interventions and enhanced surveillance. These results lay the foundation for future research and policy decisions, emphasizing the importance of strengthening vector control measures, diagnostic capacity, and public awareness. Despite these limitations, this study serves as a stepping stone for more comprehensive investigations to address knowledge gaps and develop effective strategies for combating dengue in Somaliland and similar settings. The insights gained from this research contribute to a broader understanding of dengue epidemiology in understudied regions and underscore the importance of context-specific approaches in global dengue control efforts.
Data availability
The datasets utilized in this study are not publicly accessible because of privacy concerns. However, interested parties may contact the corresponding author to request access to the data, thereby supporting the findings presented herein. Any such request is evaluated on a case-by-case basis.
Abbreviations
- DENV: Dengue virusDHF: Dengue hemorrhagic fever
DSS: Dengue shock syndrome
ELISA: Enzyme-linked immunosorbent assay
IgM: Immunoglobulin M
NS1: Non-structural protein 1
RDTs: Rapid diagnostic tests
References
-
Pierson TC, Diamond MS. Vaccine development as a means to control dengue virus pathogenesis: do we know enough? Annual Rev Virol. 2014;1(1):375–98.
-
Priyadarshi M, Sikdar S, Brijwal M. Immune Response in Dengue Fever and Clinical Implications. 2024.
-
Ekiriyagala W, Noordeen F, Pitchai F, Abeykoon A, Ariyaratne C. Abundance and dengue virus dynamics of Aedes aegypti and Aedes albopictus in selected urban areas of Kegalle and Peradeniya. Sri Lankan J Infect Dis. 2015;5(1).
-
Lin J-J, Chung P-J, Dai S-S, Tsai W-T, Lin Y-F, Kuo Y-P, et al. Aggressive organ penetration and high vector transmissibility of epidemic dengue virus-2 Cosmopolitan genotype in a transmission mouse model. PLoS Pathog. 2021;17(3):e1009480.
-
Gainor EM, Harris E, LaBeaud AD. Uncovering the burden of dengue in Africa: considerations on magnitude, misdiagnosis, and ancestry. Viruses. 2022;14(2):233.
-
Nakase T, Giovanetti M, Obolski U, Lourenço J. Population at risk of dengue virus transmission has increased due to coupled climate factors and population growth. Commun Earth Environ. 2024;5(1):475.
-
Rocklöv J, Tozan Y. Climate change and the rising infectiousness of dengue. Emerg Top Life Sci. 2019;3(2):133–42.
-
Bosa HK, Montgomery J, Kimuli I, Lutwama J. Dengue fever outbreak in Mogadishu, Somalia 2011: co-circulation of three dengue virus serotypes. Int J Infect Dis. 2014;21:3.
-
Botros BA, Watts DM, Soliman AK, Salib AW, Moussa MI, Mursal H, et al. Serological evidence of dengue fever among refugees, Hargeysa, Somalia. J Med Virol. 1989;29(2):79–81.
-
Tchuandom SB, Tchadji JC, Tchouangueu TF, Biloa MZ, Atabonkeng EP, Fumba MIM, et al. A cross-sectional study of acute dengue infection in paediatric clinics in Cameroon. BMC Public Health. 2019;19:1–7.
-
Hussien HH. Epidemiological Descriptive Analysis of Disease Outbreaks in 2019 in Sudan. Open J Epidemiol. 2020;10(04):419–31.
-
Aniakwaa-Bonsu E, Amoako-Sakyi D, Dankwa K, Prah JK, Nuvor SV. Seroprevalence of Dengue viral infection among adults attending the University of Cape Coast Hospital. Adv Infect Dis. 2021;11(01):60.
-
Fujimoto DE, Koifman S. Clinical and laboratory characteristics of patients with dengue hemorrhagic fever manifestations and their transfusion profile. Revista brasileira de hematologia e Hemoterapia. 2014;36(02):115–20.
-
Chhong LN, Poovorawan K, Hanboonkunupakarn B, Phumratanaprapin W, Soonthornworasiri N, Kittitrakul C, et al. Prevalence and clinical manifestations of dengue in older patients in Bangkok Hospital for Tropical diseases. Thail Trans Royal Soc Trop Med Hygiene. 2020;114(9):674–81.
-
Low S-L, Lam S, Wong W-Y, Teo D, Ng L-C, Tan L-K. Dengue seroprevalence of healthy adults in Singapore: serosurvey among blood donors, 2009. Am J Trop Med Hyg. 2015;93(1):40.
-
Ahmad N, Khan T, Jamal SM. A comprehensive study of dengue epidemics and persistence of anti-dengue virus antibodies in District Swat, Pakistan. Intervirology. 2020;63(1–6):46–56.
-
Malik M, Javed F, Wasim M, Ulfat M, Arshad S, Younas R, et al. Frequency of dengue virus infection among febrile patients of Lahore. Global J Health Sci. 2017;9(10):212.
-
Sharmake MA, Sultan K, Zaman QU, Rehman R, Hussain A. Decadal impacts of climate change on rainfed agriculture community in Western Somaliland. Afr Sustain. 2022;15(1):421.
-
Acosta D, Barrow A, Mahamadou IS, Assuncao VS, Edwards ME, McKune SL. Climate change and health in the Sahel: a systematic review. Royal Soc Open Sci. 2024;11(7):231602.
-
Araujo RV, Albertini MR, Costa-da-Silva AL, Suesdek L, Franceschi NCS, Bastos NM, et al. São Paulo urban heat islands have a higher incidence of dengue than other urban areas. Brazilian J Infect Dis. 2015;19(2):146–55.
-
Prestes-Carneiro LE, Barbosa Souza A, Belussi GL, Grande GHD, Bertacco EAM, Vieira AG, et al. Dengue outbreaks in a city with recent transmission in São Paulo state, Brazil. Int J Environ Health Res. 2024;34(3):1370–83.
-
Tian H, Huang S, Zhou S, Bi P, Yang Z, Li X, et al. Surface water areas significantly impacted 2014 dengue outbreaks in Guangzhou, China. Environ Res. 2016;150:299–305.
-
Man O, Kraay A, Thomas R, Trostle J, Lee GO, Robbins C, et al. Characterizing dengue transmission in rural areas: a systematic review. PLoS Negl Trop Dis. 2023;17(6):e0011333.
-
Murphy A, Rajahram GS, Jilip J, Maluda M, William T, Hu W, et al. Incidence and epidemiological features of dengue in Sabah, Malaysia. PLoS Negl Trop Dis. 2020;14(5):e0007504.
-
Telle O, Nikolay B, Kumar V, Benkimoun S, Pal R, Nagpal B, et al. Social and environmental risk factors for dengue in Delhi city: a retrospective study. PLoS Negl Trop Dis. 2021;15(2):e0009024.
-
da Conceição Araújo D, Dos Santos AD, Lima SVMA, Vaez AC, Cunha JO, de Araújo KCGM. Determining the association between dengue and social inequality factors in north-eastern Brazil: a spatial modelling. Geospat Health. 2020;15(1).
-
Ault SK. Environmental management: a re-emerging vector control strategy. Am J Trop Med Hyg. 1994;50(6 Suppl):35–49.
-
Muller DA, Depelsenaire AC, Young PR. Clinical and laboratory diagnosis of dengue virus infection. J Infect Dis. 2017;215(suppl2):S89–95.
-
Subbalaxmi M, Kumar GV, Ramanjaneyulu K, Kapoor A, Teja V, Lakshmi V. Clinical, laboratory profile and outcome of dengue fever at a south Indian tertiary care hospital. J Clin Sci Res. 2017;6(3):160–70.
-
Juliansen A, Muljono MP, Budiputri CL, Meliani F, Heriyanto RS, Chandra S et al. Clinical profile of dengue fever and dengue haemorrhagic fever in Indonesian children: a six-year retrospective study. Sri Lanka J Child Health. 2024;53(2).
-
Kumari PL. Clinical Profile and Outcome of Dengue Fever in Tertiary Care Hospital at Kerala. Acad J Med. 2020;3(2):1–5.
-
Kinoshita K, Fukuchi S, Fukuda K, Okamoto K, Ogawa R, Matsunari O, et al. A case of dengue fever that should be considered as imported infectious disease with digestive symptoms. Clin J Gastroenterol. 2021;14:1115–20.
-
Waqar K, Akhtar H, Khan MM, Umar M, Rauff B, Faheem M. A case report of dengue shock syndrome complicated with multi-organ failure and hepatitis E virus superinfection. Future Virol. 2022;17(10):717–21.
-
Carod-Artal FJ, Wichmann O, Farrar J, Gascón J. Neurological complications of dengue virus infection. Lancet Neurol. 2013;12(9):906–19.
-
Kulkarni R, Pujari S, Gupta D. Neurological manifestations of dengue fever. Ann Indian Acad Neurol. 2021;24(5):693–702.
-
Shokeen P, Yadav S, Verma CR, Masand R. Neurological complications in dengue fever. Int J Contemp Pediatr. 2018;5(3):983–7.
-
WHO. World Health Organization. (2009). Dengue guidelines for diagnosis, treatment, prevention and control: new edition. World Health Organization. https://iris.who.int/handle/10665/44188. 2009.
-
Pang J, Hsu JP, Yeo TW, Leo YS, Lye DC. Diabetes, cardiac disorders and asthma as risk factors for severe organ involvement among adult dengue patients: a matched case-control study. Sci Rep. 2017;7(1):39872.
-
Lee K, Hsieh C-J, Lee C-T, Liu J-W. Diabetic patients suffering dengue are at risk for development of dengue shock syndrome/severe dengue: emphasizing the impacts of co-existing comorbidity (ies) and glycemic control on dengue severity. J Microbiol Immunol Infect. 2020;53(1):69–78.
-
Badawy A, Sharaf H, AdelMahmoud A. Clinical and hematological effects of dengue viruses infection. Am J Infect Dis Microbiol. 2016;4:74–8.
-
Al Awaidy ST, Khamis F, Al-Zakwani I, Al Kindi S, Al Busafi S, Al Sulaimi K, et al. Epidemiological and clinical characteristics of patients with dengue fever in a recent outbreak in Oman: a single center retrospective-cohort study. Oman Med J. 2022;37(6):e452.
-
Paraná VC, Feitosa CA, da Silva GCS, Gois LL, Santos LA. Risk factors associated with severe dengue in Latin America: a systematic review and meta-analysis. Tropical Med Int Health. 2024;29(3):173–91.
-
Verhagen LM, de Groot R. Dengue in children. J Infect. 2014;69:S77–86.
-
Jama SS, Abshir SN, Jama JS, Abdi MM. Retrospective study on the dengue fever outbreak in Puntland State, Somalia. BMC Infect Dis. 2024;24(1):735.
-
Abbas I, Shalabi MG, Abbas AM, Mohamed H, Babker A, Omer AFA. Sero-prevalence of dengue fever virus antibodies in Red Sea State, Sudan-a cross-sectional study. J Pharm Res Int. 2021;33(47A):506–10.
-
Kittigul L, Pitakarnjanakul P, Sujirarat D, Siripanichgon K. The differences of clinical manifestations and laboratory findings in children and adults with dengue virus infection. J Clin Virol. 2007;39(2):76–81.
-
Siddiqui O, Chakravarti A, Abhishek KS. Dengue: lessons of an outbreak. J Clin Diagn Research: JCDR. 2016;10(6):DC01.
-
Sharma P, Pavithra K, Shettigar S. Trends in Dengue virus infection with seasonal variation at a tertiary care centre, Mangaluru: a retrospective study. IP Int J Med Microbiol Trop Dis. 2023;8(4):294–8.
-
Loconsole D, Metallo A, De Robertis AL, Morea A, Quarto M, Chironna M. Seroprevalence of dengue virus, West Nile virus, Chikungunya virus, and Zika virus in international travelers attending a travel and migration center in 2015–2017, Southern Italy. Vector-Borne Zoonotic Dis. 2018;18(6):331–4.
-
Moi ML, Omatsu T, Tajima S, Lim CK, Kotaki A, Ikeda M, et al. Detection of dengue virus nonstructural protein 1 (NS1) by using ELISA as a useful laboratory diagnostic method for dengue virus infection of international travelers. J Travel Med. 2013;20(3):185–93.
-
Datta S, Wattal C. Dengue NS1 antigen detection: a useful tool in early diagnosis of dengue virus infection. Ind J Med Microbiol. 2010;28(2):107–10.
-
Deshkar ST, Tore RP, Raut SS, Khadse RK. Ns1 Antigen Detection By Elisa In Early Laboratory Diagnosis Of Dengue Infection. 2018.
-
Biswas HH, Ortega O, Gordon A, Standish K, Balmaseda A, Kuan G, et al. Early clinical features of dengue virus infection in Nicaraguan children: a longitudinal analysis. PLoS Negl Trop Dis. 2012;6(3):e1562.
-
Hasan S, Jamdar SF, Alalowi M, Al Beaiji SMAA. Dengue virus: a global human threat: review of literature. J Int Soc Prev Community Dentistry. 2016;6(1):1–6.
-
Teixeira LAS, Nogueira FPS, Nascentes GAN. Prospective study of patients with persistent symptoms of dengue in Brazil. Revista do Instituto de Medicina Tropical de São Paulo. 2017;59:e65.
-
Tiga-Loza DC, Martínez-Vega RA, Undurraga EA, Tschampl CA, Shepard DS, Ramos-Castañeda J. Persistence of symptoms in dengue patients: a clinical cohort study. Trans R Soc Trop Med Hyg. 2020;114(5):355–64.
-
Mallhi TH, Khan AH, Adnan AS, Sarriff A, Khan YH, Jummaat F. Clinico-laboratory spectrum of dengue viral infection and risk factors associated with dengue hemorrhagic fever: a retrospective study. BMC Infect Dis. 2015;15:1–12.
-
Suppiah J, Ching S-M, Amin-Nordin S, Mat-Nor L-A, Ahmad-Najimudin N-A, Low GK-K, et al. Clinical manifestations of dengue in relation to dengue serotype and genotype in Malaysia: a retrospective observational study. PLoS Negl Trop Dis. 2018;12(9):e0006817.
-
Lovera D, Martínez-Cuellar C, Galeano F, Amarilla S, Vazquez C, Arbo A. Clinical manifestations of primary and secondary dengue in Paraguay and its relation to virus serotype. J Infect Developing Ctries. 2019;13(12):1127–34.
-
Pinto RC, Castro DBd A, BCd S, RAd VSP, CFd C, et al. Mortality predictors in patients with severe dengue in the State of Amazonas, Brazil. PLoS ONE. 2016;11(8):e0161884.
-
Idrus NL, Md Jamal S, Abu Bakar A, Embong H, Ahmad NS. Comparison of clinical and laboratory characteristics between severe and non-severe dengue in paediatrics. PLoS Negl Trop Dis. 2023;17(12):e0011839.
-
Rodrigues RS, Brum ALG, Paes MV, Póvoa TF, Basilio-de-Oliveira CA, Marchiori E, et al. Lung in dengue: computed tomography findings. PLoS ONE. 2014;9(5):e96313.
-
Rosenberger KD, Alexander N, Martinez E, Lum LC, Dempfle C-E, Junghanss T, et al. Severe dengue categories as research endpoints—results from a prospective observational study in hospitalized dengue patients. PLoS Negl Trop Dis. 2020;14(3):e0008076.
-
UK JbDL-. Somaliland climate [Available from: https://journeysbydesign.com/destinations/somaliland/when-to-go
-
Talagala T. Distributed lag nonlinear modeling approach to identify relationship between climatic factors and dengue incidence in Colombo District, Sri Lanka. Epidemiol Biostatistics Public Health. 2015;12(4).
-
Sahay S. Climatic variability and dengue risk in urban environment of Delhi (India). Urban Clim. 2018;24:863–74.
Acknowledgments
We extend our gratitude to all study participants for their kind cooperation. Additionally, we thank the University of Burao for providing the ethical approval letter necessary to conduct this research. We also thank public laboratories for their support.
Funding
Not applicable.
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Review Committee (ERC) of the University of Burao School of Postgraduate Studies and Research. The ERC waived the requirement for informed consent due to the retrospective nature of the study and the use of existing de-identified data under the approval number (Ref. No. UoB/SPGSR/18/2024). The study was conducted in accordance with relevant ethical guidelines and regulations.
Consent for publication
Not applicable.
Clinical trial number
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article
- Received:
- Accepted:
- Published:
- DOI: https://doi.org/10.1186/s12879-025-10558-6









")





{kind=link}
{kind=link}